

Abstract
A 58 years old female type2 diabetic patient was admitted to the Central Customs Hospital with chest pain lasting for two days despite parenteral nitrates and even narcotic analgetics. The patients had been admitted to the coronary care unit in Shamakhy, but despite the optimal medical treatment her chest pain hadn't resolved, Troponin I level was high (10 ng/ml), her EKG changes (ST depression) had become deeper and she had been referred to us for coronary angiography. She was extremely ill on admittio. Signs and symptoms of cardiogenic shock was present: BP was 50/20 mm Hg, with heart rate 122 bpm, she was drowsy an unresponsive, peripherally cool and diaphoretic. A five millimetres downsloping ST depression in all precordial leads was present.
Full article
A 58 years old female type2 diabetic patient was admitted to the Central Customs Hospital with chest pain lasting for two days despite parenteral nitrates and even narcotic analgetics. The patients had been admitted to the coronary care unit in Shamakhy, but despite the optimal medical treatment her chest pain hadn't resolved, Troponin I level was high (10 ng/ml), her EKG changes (ST depression) had become deeper and she had been referred to us for coronary angiography. She was extremely ill on admittio. Signs and symptoms of cardiogenic shock was present: BP was 50/20 mm Hg, with heart rate 122 bpm, she was drowsy an unresponsive, peripherally cool and diaphoretic. A five millimetres downsloping ST depression in all precordial leads was present.
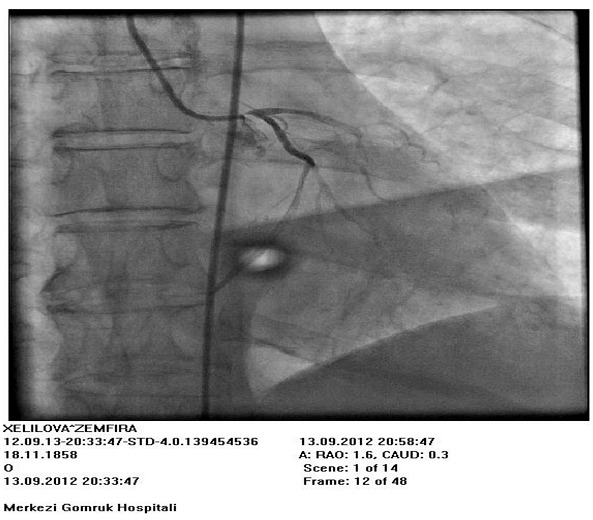
She was immedieately taken to the cath lab, and in first injection to the left coronary system a subtotal ostial occlusion of the left main coronary artery was observed. (fig1). At this moment pulmonary arrest was documented, arterial systolic pressure was 30 mm Hg. Cardiopulmonary resuscitation was started. Due to the critical condition and no time for preparation the patient to operation, it was decided to stent the left main ostium. Intravenous dopamin was started, an intraaortic balloon pump was inserted through the left groin and countrapulsation at a 2:1 ratio with 100 % augmentation was started. 10.000 IU of unfractionated heparin was given intravenousely. Then LMCA was intubated with 6F JL4 guiding catheter, already having PT2 0.014'' guidewire and 2.0x12 mm Sprinter Legend coronary balloon catheter in it, because we had no time for consequent steps after intubation of the Left Main. A lesion was crossed with guidewire and dilated with balloon, then 2.5x18 mm Zotarolimus Eluting Stent was implanted from the left main coronary artery ostium to the proximal LAD - a simple cross-over technique - at 22 Atm. The lesion was completely expanded with good angographic result. (fig2). The right coronary angiogramm was obtained at this moment-it was non-dominant with no any abnormality. The patient's hymodynamics was quickly and completely restored, chest pain resolved and EKG changes became better within an hour and completely resolved the next day. An intraaortic balloon pump keeped in for 24 hours, then had been removed. A standart dual antiplatelet treatment, statin and beta blockers were started and the patient was discharged after 4 days in good health without any complaints. She remains good in 30 days after intervention.
Discussion : This is the case of rare emergent intervention to the left main trunk due to the critical condition (cardiogenic shock) of the patient with acute NSTEMI. Despite the fact that in some centers elective interventions on left main coronary artery are being performing, coronary artery bypass grafting surgery is still a method of choice in such situations, and LMCA intervention has only IIB indication (level of evidence C) and only in selected patients. So in our center we do not perform elective left main interventions, only to patients amenable to surgical treatment due to co-morbidities or surgical refusees. Numerous registries and nonrandomized comparative trials have shown feasibility, relative safety and efficacy of left main stenting using both bare metal and drug-eluting stents. LEft main stem stenting is a high-risk lesion subset for several reasons. First; the left main stem supplies a very large vascular territory and there is the potential for cardiovascular collapse with ischemia; particularly if the left coronary is dominant (such in our case), the right coronary is occluded, or left ventricular function is reduced. Left main stem disease involves the bifurcation in more thanhalf the cases, introducing additional complexity and risk. Finally, the occurence of either restenosis or stent thrombosis may be fatal events in patients with left main stents. But in such patients with acute coronary syndrome complicated with acute heart failure and even cardiogenic shock, emergent and rapid revascularisation with percutaneous approach is life-saving and should be performed instead of time-consuming preparation of patient to the surgery which might put the patient in more risk.
Conclusion: The simple cross over approach should be chosen during intervention in left main trunk in such acutely ill patients without complicated bifurcation techniques. An intraaortic balloon pump should be used as widely as possible if there are no contraindications. "The simpler the better". The main goal is restoration of TIMI-3 flow in all major branches. Complex bifurcation stenting during emergency PCI for left main occlusion is not advisable.
Figures

Keywords
References
1. Results and Long-Term Predictors of Adverse Clinical Events After Elective Percutaneous Interventions on Unprotected Left Main Coronary Artery .Takuro Takagi, G Stankovic, L Finci, K Toutouzas, A Chieffo and etc. Circulation.2002
2. Short- and Long-Term Clinical Outcome After Drug-Eluting Stent Implantation for the Percutaneous Treatment of Left Main Coronary Artery Disease Insights From the Rapamycin-Eluting and Taxus Stent Evaluated At Rotterdam Cardiology Hospital Registries (RESEARCH and T-SEARCH).M Valgimigli, CAG van Mieghem, ATL Ong, J Aoki… - Circulation, 2005 - Am Heart Assoc
3. Taggart DP, Kaul S, Boden WE, Ferguson TB et al: Revascularization for unprotected left main stem coronary artery stenosis: Stenting or surgery, J Am Coll Cardiol 51:885-892, 2008.
Article Info:
Publication history
Published: 10.Apr.2012
Copyright
© 2013-2025. Azerbaijan Society of Cardiology. Published by "Uptodate in Medicine" health sciences publishing. All rights reserved.Related Articles
Viewed: 2038