

Abstrakt
Giriş: Kardiovaskulyar görüntüləmə texnikalarının təkmilləşdirilməsi, xüsusilə invaziv koronar angioqrafiya və koronar KT angioqrafiyanın geniş tətbiqi bizə koronar anatomiya, koronar anomaliyalar, koronar dominantlıq və onların xəstələrin ölüm və xəstələnmə səviyyəsinə təsiri haqqında çoxlu yeni məlumatlar vermişdir. Koronar arteriya dominantlığı, interventrikulyar septumun aşağı hissəsini qanla təchiz edən arxa enən arteriyaya (PDA) başlanğıc verən koronar arteriyaya əsasən müəyyən edilir. Material və metodlar: Biz tədqiqata 01.10.2021 və 30.10-2021-ci il tarixləri arasında klinikamıza kəskin koronar sindrom (KKS) və gərginlik stenokardiyası ilə müraciət etmiş 1178 xəstəni daxil etmişik. Nəticələr: Xəstələrimizin 68%-i (N 802) RCA dominantlığına, 27.5%-i (N 326) Cx dominantlığına və 4.5%-i (N50) kodominantlığa malik idi. Kohortumuzun 1,9% -ində əzələ körpüləri, 2,7% -də koronar yavaş axın fenomeni, 5,1% -də ana koronar arteriyanın olmaması, 5,9% -də intermediat arteriya və 5,6% -də koronar arteriyalarda tortuozluq var idi. Biz bütün kohortun 0,08%-ni təşkil edən 1 xəstədə tək koronar arteriya müşahidə etdik, xəstələrin 0,16%-də koronar ostiumun əks sinusdan anomal çıxışını müşahidə etdik. Yekun: Nəticə olaraq, bizim kohortumuzda xəstələrin 68%-də RCA dominantlığı, 27.6%-də Cx dominantlığı və 4.4%-də kodominantlıq var idi ki, bu nəticələr də əvvəlki araşdırmaların nəticələrinə yaxındır.
Əsas mətn
Introduction: Coronary artery disease is the most common cause of morbidity and mortality in the world. Improving cardiovascular imaging techniques, especially the widespread usage of invasive coronary angiography and coronary CT angiography, give us a lot of information about coronary anatomy, coronary anomalies, coronary dominancy, and the impact of these on the mortality and morbidity of patients. Coronary artery dominance is defined by the vessel that gives rise to the posterior descending artery (PDA), which supplies the inferior part of the interventricular septum. Dominance has important implications for myocardial ischemia and infarction. Tortuosity is one of the issues that complicates coronary interventions. Some forms of coronary anomalies make coronary angiography and coronary interventions difficult for the operator. Some of them increase morbidity and mortality (for instance, the interarterial course of the left anterior descending artery).
Material and methods: From October 1, 2021, to October 30, 2021, we enrolled 1178 patients who underwent coronary angiography in our hospital for the acute coronary syndrome (ACS) and chronic coronary syndrome (CCS). Angiograms obtained under an invasive coronary angiogram Invasive procedures have been performed in our center for more than 20 years. The results were evaluated by 3 independent interventional cardiologists with at least 10 years of experience in interventional cardiology. We used Angelini's CAA classification method to classify anomalies. We used TIMI flow counting to identify the coronary slow flow phenomenon (1.7 correction factor for the left anterior descending artery was used)1. The patients' data were hidden from researchers, and patient data were downloaded anonymously from the angiography device archive. Research ethic committee of the national Cardiac Society of Azerbaijan approved our research.
Statistical Analysis. Research data were transferred to a computer and analyzed using IMB SPSS statistics for Windows version 18.0 (IBM. Crop.,Armonk, NY, USA). We used categorical variables and expressed them as percentages. Chi-square and independent the sample t-test were used.
Results: 68 % (N 802) of our patients had RCA, 27 % (N 326) had Cx dominancy, and 4.5 percent (N 50) were found to have codominancy. The mean age of patients was 66 years, whereas the youngest patient was 30 years old and the oldest patient was 81 years old. 91 (11.4%) patients out of 802 in a RCA dominancy group were women, and 711 of them (88.5%) were men. 5 (2%) of the 50 people in the codominancy group were women, while 46 (98%) were men.78 (23.9%) patients out of 326 in the CX dominancy group were women, and 248 (76.1%) of them were men (Table 1).
See pdf. Table 1 . Sex differences (RCA-right coronary artery, Cx-circumflex artery)
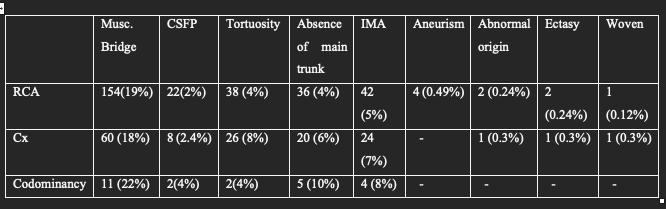
In addition to dominancy, we looked at the prevalence of myocardial bridging, coronary artery anomalies, coronary aneurisms, coronary slow flow phenomenon, tortuosity, and the presence of the intermediate artery (IMA) in our population.
In the right coronary artery dominancy group, there were 154 (19%) patients with muscular bridges. 152 of them were in the left anterior descending coronary artery, and 2 of them were in the circumflex artery. There was an absence of the main trunk (absence of the left main coronary artery) in 36 (4%) patients, with the right and left coronary arteries emerging from the left sinus of Valsalva separately. 42 (5%) patients had an intermediate artery arising from the left main coronary artery. 4 (0.49%) patients had aneurisms in the left anterior decending artery.
In the RCA dominancy group, 2% (N 22) of patients had coronary slow flow phenomenon.
We found two (0.24%) patients with an abnormal location of the coronary ostium in an incorrect sinus (in one patient, the RCA originated from the left sinus of Valsalva, and in another, the CX originated from the right sinus of Valsalva).
2 (0.24%) patients had ectatic coronary arteries, and a (0.12%) patient had woven formation in the LAD. 38 (4%) patients had mid-to-distal tortuosity in all 3 coronary arteries (Table 2). In the left coronary artery dominancy (Cx dominancy) group there were 60 (18%) patients with muscular bridges. All of them were in the left anterior descending coronary artery. In 20 (6%) patients there was an absence of main trunk (absence of left main coronary artery) in whom right and left coronary arteries took place separately from the left sinus of Valsalva. 24 (7%) patients had intermediate artery arising from the left main coronary artery. The 2.4 % (N 8) of patients had coronary slow flow phenomenon in the RCA dominancy group. We noticed a (0.3%) patient with single coronary artery, which located in the right sinus of Valsalva. 1 (0.3%) patient had ectatic coronary arteries, and 1 (0.3%) patient had woven formation in Cx. 26 (8%) patients had mid to distal tortuosity in all of 3 coronary arteries. In the codominancy group there were 11 (22%) out of 50 patients with muscular bridges. 1 of them were in Cx and another 10 in LAD. 4 patients (8%) had intermediate artery. In 5 patients (10%) there was absence of left main coronary artery. 2 (4%) patients had coronary slow phenomenon. 2 (4%) out of 50 patients had tortuosity in mid to distal parts of all 3 coronary arteries.
See pdf: Table 2. Percentage of variables in each group (RCA-right coronary artery, Cx-circumflex artery, CSFP-coronary slow flow phenomenon, IMA-intermediate artery)
To sum up, the 1.9% of our population had muscular bridges, 2.7% had coronary slow flow phenomenon, 5.1% had the absence of main trunk, 5.9% had the presence of intermediate artery and 5.6% had tortuosity in coronary arteries. We observed in a patient single coronary artery which is the 0.08 % of all population, in 0.16% of patients there was an anomalous location of coronary ostium in improper sinus.
Discussion. Coronary artery dominancy has an approximately similar distribution in most countries and among most nations. We also tried to investigate the distribution in our patients. In another study, out of 52 undissected isolated cadaveric hearts, the right cardiac dominance was found in 42 (80.76%). 2. In South India, right cardiac dominance was seen in 85.5% of cases, left in 9.7%, and co-dominant in 4.8% of cases. 3. In another single center study, RCA dominance was in 70.99% (N = 5579), Cx dominance was 12.99% (N = 1021) , and codominancy was in 16.01% (N = 1258) patients 4. In our cohort, RCA dominancy was lower and Cx dominancy was higher than previously reported. In our opinion genetic or geographical factors can contribute to this discrepancy.
Azerbaijan has a population of about 10, 000,000 people. The sample size, in our opinion, was insufficient to accurately represent the prevalence or dominance of coronary anomalies. But of course, this sample was not enough to detect the different ranges of coronary anomalies. A larger sample size may be needed for this.
Conclusion: In conclusion, in our cohort, the 68% of patients had RCA dominancy, 27.6% of patients had Cx dominancy, and 4.4% of patients had codominancy, which is close to previous reports.
Şəkillər

Açar sözlər
İstinadlar

Beltrame JF.
Defining the coronary slow flow phenomenon. Circ J. 2012;76(4):818-20. doi: 10.1253/circj.cj-12-0205. Epub 2012 Feb 25. PMID: 22374148.
Aricatt DP, Prabhu A, Avadhani R, Subramanyam K, Manzil AS, Ezhilan J, Das R.
A study of coronary dominance and its clinical significance. Folia Morphol (Warsz). 2022 Jan 31. doi: 10.5603/FM.a2022.0005. Epub ahead of print. PMID: 35099044.
Tiwari N, Budhathoki D.
Right Coronary Artery Dominance in Cadaveric Human Hearts in Department of Anatomy of a Medical College: A Descriptive Cross-sectional Study. JNMA J Nepal Med Assoc. 2022 Apr 15;60(248):374-376. doi: 10.31729/jnma.7432. PMID: 35633210; PMCID: PMC9252237.
Akkaya H, Güntürk EE.
Coronary artery anomalies and dominance: data from a single center in Turkey. Minerva Cardiol Angiol. 2022 Apr;70(2):138-147. doi: 10.23736/S2724-5683.20.05279-2. Epub 2020 Sep 29. PMID: 32989969.
Məqalə barədə təfərrüatlar:
Nəşr tarixçəsi
Dərc edilib: 14.Oct.2023
Müəllif hüququ
© 2013-2025. Azərbaycan Kardiologiya Cəmiyyətinin rəsmi nəşri. Jurnal "Uptodate in Medicine" tibb nəşriyyatı tərəfindən dərc olunur. Bütün hüquqlar qorunur.Əlaqəli məqalələr
Baxılıb: 2530